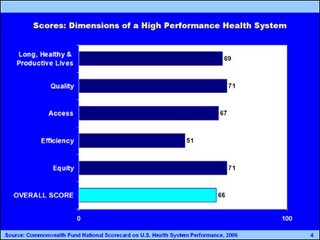
Across 37 indicators of performance, the U.S. achieves an overall score of 66 out of a possible 100 when comparing actual performance to achievable benchmarks, or a "D+". The following graph shows the score for the US in the major areas observed.
Click Graph to Enlarge
 These results clearly show that not only is cost a problem, and not only do we have about 45 million people who are not covered, but our results for the money spent fall far short of what is needed and achieveable.
These results clearly show that not only is cost a problem, and not only do we have about 45 million people who are not covered, but our results for the money spent fall far short of what is needed and achieveable.
I have included a link to the report in this blog, but I believe that the messages from the Scorecard are clear:
Preventive and primary care quality deficiencies undermine outcomes for patients and contribute to inefficiencies that raise the cost of care. These deficiencies are to be expected in a system that chronically underfunds primary care, and does not pay doctors for proven primary care strategies such as electronic medical records, chronic disease registries, telephone management followup, web messaging and quality benchmarks. Universal coverage and participation are essential to improve quality and efficiency, as well as access to needed care.
Quality and efficiency can be improved together, and we must look for improvements that yield both results. Failure to coordinate care for patients over the course of treatment put patients at risk and raise the cost of care. This is especially acute with patients who do not have a "Personal medical home". Policies that facilitate and promote linking providers and information about care will be essential for productivity, safety, and quality gains. Financial incentives posed by the fee-for-service system of payment as currently designed undermine efforts to improve preventive and primary care, manage chronic conditions, and coordinate care. We need to devise payment incentives to reward more effective and efficient care, with a focus on value. Research and investment in data systems are important keys to progress. Investment in, and implementation of, electronic medical records and modern health information technology in physician offices and hospitals is low—leaving physicians and other providers without useful tools to ensure reliable high quality care. By emphasizing adequate payment for primary care, savings can be generated from more efficient use of expensive resources including more effective care in the community to control chronic disease and assure patients timely access to primary care. The challenge is finding ways to re-channel these savings into investments in improved coverage and system capacity to improve performance in the future.
Setting national goals for improvement based on best achieved rates is likely to be an effective method to motivate change and move the overall distribution to higher levels.
Our health system needs to focus on improving health outcomes for people over the course of their lives, as they move from place to place and from one site of care to another. This requires a degree of organization and coordination that we currently lack. It also requires that each person have a "personal medical home" with a primary care physician office team.
This Scorecard is a snap shot of the vital signs of our health system. It is not a pretty picture! Our rising costs and deteriorating coverage require leadership to transform the health system.
I say, let's start by adequately funding all primary care, so that we begin with the basics - adequate access for early care, chronic disease care and preventive care. This personal medical home, supported by state of the art medical records, can then be the organizing central point for improving communication and reforming the health care system.
 These results clearly show that not only is cost a problem, and not only do we have about 45 million people who are not covered, but our results for the money spent fall far short of what is needed and achieveable.
These results clearly show that not only is cost a problem, and not only do we have about 45 million people who are not covered, but our results for the money spent fall far short of what is needed and achieveable.I have included a link to the report in this blog, but I believe that the messages from the Scorecard are clear:
Preventive and primary care quality deficiencies undermine outcomes for patients and contribute to inefficiencies that raise the cost of care. These deficiencies are to be expected in a system that chronically underfunds primary care, and does not pay doctors for proven primary care strategies such as electronic medical records, chronic disease registries, telephone management followup, web messaging and quality benchmarks. Universal coverage and participation are essential to improve quality and efficiency, as well as access to needed care.
Quality and efficiency can be improved together, and we must look for improvements that yield both results. Failure to coordinate care for patients over the course of treatment put patients at risk and raise the cost of care. This is especially acute with patients who do not have a "Personal medical home". Policies that facilitate and promote linking providers and information about care will be essential for productivity, safety, and quality gains. Financial incentives posed by the fee-for-service system of payment as currently designed undermine efforts to improve preventive and primary care, manage chronic conditions, and coordinate care. We need to devise payment incentives to reward more effective and efficient care, with a focus on value. Research and investment in data systems are important keys to progress. Investment in, and implementation of, electronic medical records and modern health information technology in physician offices and hospitals is low—leaving physicians and other providers without useful tools to ensure reliable high quality care. By emphasizing adequate payment for primary care, savings can be generated from more efficient use of expensive resources including more effective care in the community to control chronic disease and assure patients timely access to primary care. The challenge is finding ways to re-channel these savings into investments in improved coverage and system capacity to improve performance in the future.
Setting national goals for improvement based on best achieved rates is likely to be an effective method to motivate change and move the overall distribution to higher levels.
Our health system needs to focus on improving health outcomes for people over the course of their lives, as they move from place to place and from one site of care to another. This requires a degree of organization and coordination that we currently lack. It also requires that each person have a "personal medical home" with a primary care physician office team.
This Scorecard is a snap shot of the vital signs of our health system. It is not a pretty picture! Our rising costs and deteriorating coverage require leadership to transform the health system.
I say, let's start by adequately funding all primary care, so that we begin with the basics - adequate access for early care, chronic disease care and preventive care. This personal medical home, supported by state of the art medical records, can then be the organizing central point for improving communication and reforming the health care system.
No comments:
Post a Comment