One of my favorite and most useful resources for understanding the complexity and variation in our United States health care "system" is the Dartmouth Atlas of Health Care.
One of the most fascinating observations made as a result of this ongoing study was published in 2004 (Health Affairs, 10.1377/hlthaff.w4.184 Copyright © 2004 by Project HOPE ). The authors, Katherine Baicker and Amitabh Chandra studied the relationship between Medicare Spending, the type of physician workforce, and beneficiary's quality of care. The results were astounding, and showed that only one parameter correlated with improved quality and decreased cost, and that was the ratio of family physicians to the general population.
Click to Enlarge
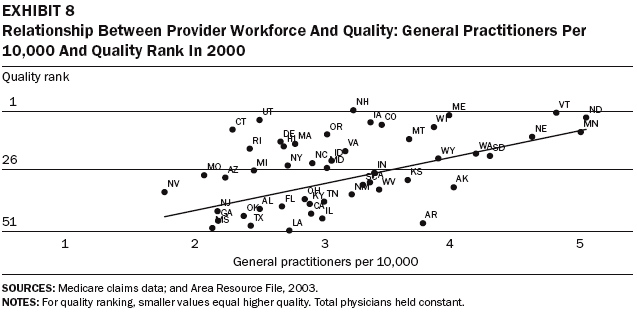
 These results confirm what has also noted all over the world, which is that high functioning health care systems have a high ratio of primary care doctors as part of the physician work force. The authors also looked at the affect of the ratio of more narrowly focused specialist physicians on cost and quality.
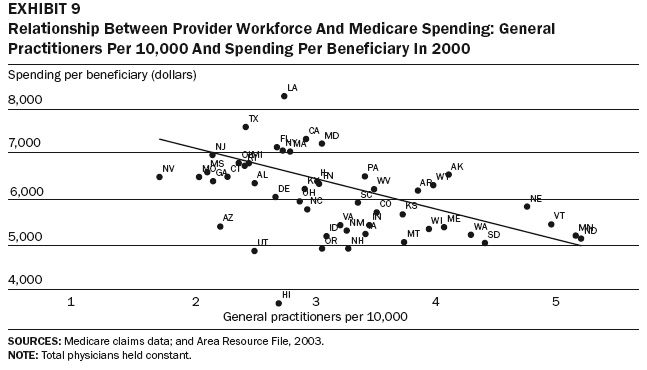
These results confirm what has also noted all over the world, which is that high functioning health care systems have a high ratio of primary care doctors as part of the physician work force. The authors also looked at the affect of the ratio of more narrowly focused specialist physicians on cost and quality.Click to Enlarge

 The data clearly show that as the ratio of narrowly focused specialist doctors increases relative to the general population, cost goes up and overall quality actually worsens!
The data clearly show that as the ratio of narrowly focused specialist doctors increases relative to the general population, cost goes up and overall quality actually worsens!How can this be? It seems counter intuitive to many people that more specialists would result in lower quality of care. Based on my years of practice experience, I believe these results are accurate, and that the results are due to several factors:
1.) When family physicians are in short supply, needed primary care services, that should be the foundation of all that we do, are not received by many people who have their first contact with specialists .
2.) When family physicians are in short supply, they are forced into a mode of seeing patients more quickly than is desirable, which I believe lowers the quality and the patient satisfaction. Costs go up because it is easier to simply order the expensive tests that drive up costs than it is to do a detailed history and physical exam before planning workup.
3.) Due to their training and focus, narrowly trained specialists sometimes bring high risk and high expense habits to bear in situations where a less aggressive approach might be preferable.
These doctors are a valuable and needed part of our care delivery system, but they do not specialize in first access health care, screening and helping us to stay well.
The authors looked at other factors, but did not observe any other clear relationships. Data on nurses, for example, did not show a change with a changing ratio to population.
Click to Enlarge
 So what does this mean for health care reform? To me, the implications are clear, and aggressive action is required. Health insurers and the federal government need to begin immediately to implement policies that nurture the provision of primary care.
So what does this mean for health care reform? To me, the implications are clear, and aggressive action is required. Health insurers and the federal government need to begin immediately to implement policies that nurture the provision of primary care.Unfortunately, the current state of affairs is bleak. The American College of Physicians (ACP) has issued a 2006 report that predicts the imminent collapse of primary care in the United States, due to the inadequate and dysfunctional payment policies of the government and other third party payers. Most government payment programs do not even cover the overhead cost of doctors to provide primary care, and the situation is getting worse! Medicare, for example, is scheduled to decrease payments by 5.1% as of January, 2007. Fewer and fewer medical students are choosing to pursue family medicine or other primary care as a career option, because they know they can make more money at less personal risk by going into a high tech, limited specialty. Many existing primary care doctors are near retirement and will soon be out of the workforce. And all of this is happening at the very time we will experience a large jump in Medicare age patients needing primary care services.
The Medicare situation is due to the way payments to doctors are calculated. Medicare Part "B" was established to cover doctors visits. As care has become more technical and complex, new services have been added into the pot for coverage. Now, in addition to doctors visits, Par "B" also covers out patient surgery, CT scans, MRI scans, nuclear medicine and other high tech wonders. This then results in Medicare Part "B" spending "too much money", and payment reductions for everyone are then put in place. Primary care office visits get cut back, in spite of the fact that payment is already too low.
If we began a national policy of enhancing the ability of family physicians to provide excellent primary care, it would need to start by decoupling primary care payment from the rest of payment for health care. This would encourage the development of what the American Academy of Family Physicians (AAFP) calls the "personal medical home", a place where they know your name and each of us knows we can go for care and referral. Payment to primary care practices needs to be enough to cover overhead, build state of the art infrastructure to incorporate electronic medical records, support advanced management strategies and let the doctors make a reasonable profit. This will attract doctors to family medicine at the time we need them most! The data are clear. We need to nurture and encourage the only part of our current health care "system" that is already demonstrating a clear relationship to increased quality and lower cost.
1 comment:
What an excellent, not to mention timely web-log! If only more physicians were explaining about the system from THEIR perspective - you're doing truly great, pioneering work. I look forward to checking back in frequently!
Post a Comment